
貧窮, 無知, 健康不佳和營養不良陷阱母親和嬰兒的惡性循環根據孕產婦和兒童健康和營養研討會在新興市場所發生的綠鄧普頓大學的調查結果生活, 今年牛津大學早期.
每個孩子都應該有生活中的平等起步. 然而,數以百萬計的兒童在新興市場不. 一個突破性的新的多種族研究的初步結果, 共生-21, 由蓋茨基金會資助, 顯示,胎兒的生長發育決定的更多的社會, 經濟, 營養和母親的環境條件前和懷孕,而不是母親的國籍和種族中. 在共生-21的發現激發新的見解政府如何, 私營部門和民間社會可以在全球水平的健康, 發展, 發展打了場嬰兒和兒童族群在所有國家中的第一個 1000 受孕後幾天.
今天 全球搜索教育, 我們將聽到更多關於這些問題和大家分享一些對孕產婦和兒童健康和營養的新興市場提供了研討會的建議. 我很高興地歡迎喬治·阿萊恩爵士 (校長, 西印度群島大學), 崇梅城 (普林斯頓會議的聯合創始人), 卡羅琳秋季 (教授, 國際兒科流行病學, 南安普敦大學, 英國), 州長瑪德琳獲取 (新女權主義議程的作者, 定義的下一次革命的女性, 工作和家庭), 人氣選手Nishtar (創始人兼總裁, Healthfile, 巴基斯坦), 與Srinath雷迪 (總統, 印度健康基金會).


獲取省長: 能否請您總結一下關於第一個至關重要的新證據 1,000 生活的日子. 什麼是貧窮和富裕國家的影響?
已經有顯著減少世界各地的孕產婦和嬰兒死亡率. 更多的生命可以被保存,如果我們能夠利用的研究,通知我們,第一千天嬰兒的生命是成人至關重要福祉. 良好的營養和醫療保健為母親起到至關重要的作用受精發生之前很久. 再也不能分開,我們從環境遺傳學,因為母親的基因可能因營養不良影響. 我們學到的教訓告訴我們,最好的投資國可以在良好的孕產婦和嬰幼兒保健. 這不僅會挽救生命; 它會幫助產生健康的和富有成效的成年人的社會.
卡羅琳秋季: 我們知道什麼對孕產婦和兒童健康和營養 (CHN), 然而仍有交付的持續性故障. 所涉及的因素?
幾乎每個人都在誰擁有手術世界得到一個有效的麻醉劑. 這是因為,麻醉是一個相對簡單的, 簡要, 並經管一份高薪的專業直接治療, 而且是直接的明顯的好處向所有關心. 數以百萬計的母親和兒童的營養不良仍然是因為確保良好的產婦的營養和良好的懷孕和育兒很複雜,需要多個部門,多年來齊心協力. 產婦營養不良造成一些眼前的問題, 與政策制定者可能真的是無知的對胎兒和嬰幼兒發育遲緩的影響深遠的後果. 他們可能真的是不知道孩子的大腦永遠彌補赤字和孩子注定要成為一個更病態的和非生產性成人. 的主要障礙是缺乏長遠眼光和政治意願 — 意志來組織食品供應, 教育女孩和婦女, 並建立和維護一個熟練和激勵婦幼衛生人員.


人氣選手Nishtar: 為孕產婦和兒童營養不良主要是貧困問題和糧食短缺, 營養食品可用性差, 或教育和窮人的選擇缺乏? 你有什麼要解決的根本問題的最有效途徑視圖?
這是所有這些因素的組合, 雖然受金融准入門檻所起的作用是最顯著的. 因素,如貧困的影響, 產婦識字, 衛生, 而對兒童健康的住房條件和, 反過來, 對社會和經濟成果, 是有據可查的. 問題是,這些因素不適合孤立的公共衛生干預措施. 但另一個, 少廣泛討論的社會決定因素 — 孕婦營養 – 可能是. 好消息是,有解決方案. 有條件的現金轉移, 短信為基礎的舉措, 以學校為基礎的食品計劃, 維生素強化計劃, 和當地的領導都在改善孕產婦營養證明是有效的. 這些舉措應該由積極的促進營養的選擇策略進行備份. 引人注目的政策制定者們實施這些政策將需要一套新的技能,吸取了經驗教訓來自世界各地的. 倡議旨在加強營養公眾的知識也很關鍵 — 這不僅是因為他們能激勵公民迫使其政府採取行動.
崇梅城: 作為MCHN危機的圖示, 什麼樣的挑戰,必須解決中國做顯著的進步, 而且什麼樣的戰略,他們目前正在?
在中國的孕產婦和兒童健康和營養都被中國的主要受益者 1978 改革開放. 迎來了一段經濟高速增長的改革 10 在一年的大部分那段%的, 特別是在 1990-2010. 之間 1990 和 2010, 嬰兒死亡率,並在五年死亡率下降 70.5 %,而 69.8 百分, 分別, 和體重兒童的患病率 50 百分. 產婦死亡率下降 56 %之間 2000 和 2013, 和 92 所有孕婦接受百分之胎教.
顯著, nine-year universal education during this period also vastly raised the ability of the Chinese “母親,” chief nurturer of the family, to properly care for her children. 挑戰, 但, 留. Rural Chinese children, especially those living in poorer inland and western provinces, still bear a disproportionate burden of growth-related problems. Stunting and underweight prevalence in central and western China is two to three times higher than richer eastern China. Rates of stunting and being underweight among the estimated 15 million children of China’s vast population of migrant workers who are left behind in the villages are one-and-a-half times those of their non-left-behind counterparts. 而且, by the Chinese government’s own account, the infrastructure to improve rural child nutrition is still fragile, unstable, and vulnerable to changes in economic conditions. Also worrisome are the worsening trends in stunting and underweight prevalence since the 2008 financial crisis, and the toll that environmental pollution has taken and is continuing to take on all Chinese, including children who are more vulnerable to the harms that environmental degradation causes. 展望未來, China’s slower economic growth today, and in the foreseeable future are likely to exacerbate the problems of Chinese children’s health and nutrition. 幸好, China’s top policymakers are aware of the problems and have acted on them. 例如, 在 2011, China’s State Council issued the “Concise Outline of Child Development in China 2011-2020,” making improvement of maternal and child nutrition an important government mission and part of the 12th five-year plan. The specific goals are to reduce stunting, underweight and anemia prevalence among Chinese children. Some specific measures include strengthening health education and maintenance of women and children including teaching of knowledge about nutrition, and building comprehensive child nutrition monitoring programs. The Chinese government has decided to treat child nutrition improvement as a strategic mission in raising the quality of the Chinese people.


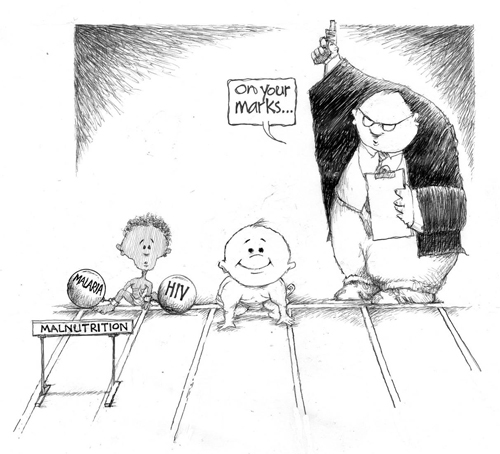
喬治·阿萊恩爵士: How do you see the progress with MCHN compared with progress in other basic human rights, such as literacy, and compared to the progress on major health problems, such as AIDS?
Recent years have seen remarkable progress in MCHN both in terms of the science of child growth and development, and in the programs and policies to be applied. There has been renewed and heightened interest in the past decade, partly because of the appreciation of the long term sequelae for health, 教育, the economy and social services of childhood malnutrition and stunting. There are technologies available for even more rapid advance if only the health services were adequate to deliver them effectively. The progress in this area has been as substantial as in the field of HIV, although the light of popular interest does not shine as brightly on the problems of mothers and children, which do not seem so dramatic.
Srinath雷迪: What are the largest MCHN challenges for India, and what strategies are most effective in your view?
Despite an accelerated rate of decline over the last decade, India’s aggregate national rates of maternal and infant mortality remain higher than those of her economic peers and even of several South Asian neighbors. The present rates (42 到 1000 live births for IMR and 178 到 100000 live births for MMR) fall short of the targets proposed in the Millennium Development Goals of 2000. Hidden within these numbers are huge inequities between different population groups, determined by region, income, education and caste. The high rates of maternal and neonatal mortality are partly responsive to the national program for increasing the demand for institutional deliveries. 然而, substantive impact can only be achieved if the quality of services provided in primary and secondary health care facilities is improved through a supply side response that provides skilled personnel, adequate infrastructure and assured availability of medicines. Efforts to reduce child mortality under 5 years must improve immunization coverage, 衛生, potable water supply, and primary care for acute respiratory infections and diarrheal diseases. Under-nutrition in childhood (an appalling 42percent) must be reduced not only to protect physical and cognitive growth but also to prevent susceptibility to both childhood infections and chronic diseases in later adulthood.


All Photos are courtesy of Green Templeton College, 牛津大學
![]()
在全球搜索教育, 和我一樣,全球知名的思想領袖,包括邁克爾·巴伯爵士 (英國), 博士. 邁克爾座 (美國), 博士. 萊昂特司特因 (美國), 克萊克里斯坦森教授 (美國), 博士. 琳達·達林 - 哈蒙德 (美國), 博士. 馬達夫恰範 (印度), 邁克爾·富蘭教授 (加拿大), 霍華德·加德納教授 (美國), 安迪·哈格里夫斯教授 (美國), 伊馮娜赫爾曼教授 (荷蘭), 克里斯汀Helstad教授 (挪威), 讓·亨德里克森 (美國), 玫瑰Hipkins教授 (新西蘭), 科妮莉亞Hoogland教授 (加拿大), 這位傑夫·約翰遜 (加拿大), 太太. 尚塔爾考夫曼 (比利時), 博士. Eija Kauppinen (芬蘭), 國務秘書塔皮奧Kosunen (芬蘭), 多米尼克·拉方丹教授 (比利時), 休·勞德教授 (英國), 本·萊文教授 (加拿大), 主肯麥克唐納 (英國), 巴里McGaw教授 (澳大利亞), 希夫納達爾 (印度), Ř教授. 納塔拉詹 (印度), 博士. 吳PAK (新加坡), 博士. 丹尼斯教皇 (美國), 斯瑞達拉賈戈帕蘭 (印度), 博士. 黛安·拉維奇 (美國), 理查德·威爾遜·賴利 (美國), 肯·羅賓遜爵士 (英國), 帕西SAHLBERG教授 (芬蘭), 押尾佐藤教授 (日本), 安德烈亞斯·施萊歇 (PISA, 經合組織), 博士. 安東尼·塞爾頓 (英國), 博士. 大衛·謝弗 (美國), 博士. 基爾斯滕都沉浸式 (挪威), 總理斯蒂芬·SPAHN (美國), 伊夫Theze (法國公立高中美國), 查爾斯Ungerleider教授 (加拿大), 托尼·瓦格納教授 (美國), 大衛·沃森爵士 (英國), 迪倫Wiliam教授 (英國), 博士. 馬克沃莫爾德 (英國), 西奧Wubbels教授 (荷蘭), 邁克爾·楊教授 (英國), 和張民選教授 (中國) 因為他們探索所有國家今天面臨的大畫面的教育問題.
全球搜索教育社區頁面
ç. M. 魯賓是兩個廣為傳誦的在線系列,她接受了筆者 2011 厄普頓·辛克萊獎, “全球搜索教育” 和 “我們將如何閱讀?” 她也是三本暢銷書, 其中 真正的愛麗絲夢遊仙境, 是的發行 CMRubinWorld, 而且是干擾物基金會研究員.
按照ç. M. 魯賓在Twitter: www.twitter.com/@cmrubinworld



最新評論